

HYPERTENSION PREVALENCE
Currently 23% of Canadian adults have hypertension and this translates to more than 40% of adults aged 25 years and older worldwide. Hypertension is currently the leading global risk factor for death/disability. However, blood pressure control has grown significantly both in Canada and globally due to advancements in pharmacotherapy. For historical context, in 1992, there was only 13.2% control of hypertensive patients in Canada. This has now grown to control of 68.1% of all hypertensive patients in 2013. Globally, there is 32.5% control of hypertensive patients worldwide. It is also worth noting that 8/10 hypertensive patients have 1 or more cardiovascular risk factors.
RISKS OF UNCONTROLLED / UNTREATED HYPERTENSION
In having discussions with patients about the importance of hypertension, it is important to keep in mind the many complications and consequences which can arise in not treating/controlling hypertension. Some of these sequalae of hypertension include cerebrovascular disease, dementia, retinopathy, coronary artery disease, heart failure, atrial fibrillation, left ventricular hypertrophy, chronic kidney disease, erectile dysfunction, and peripheral artery disease.
RISK FACTORS FOR HYPERTENSION
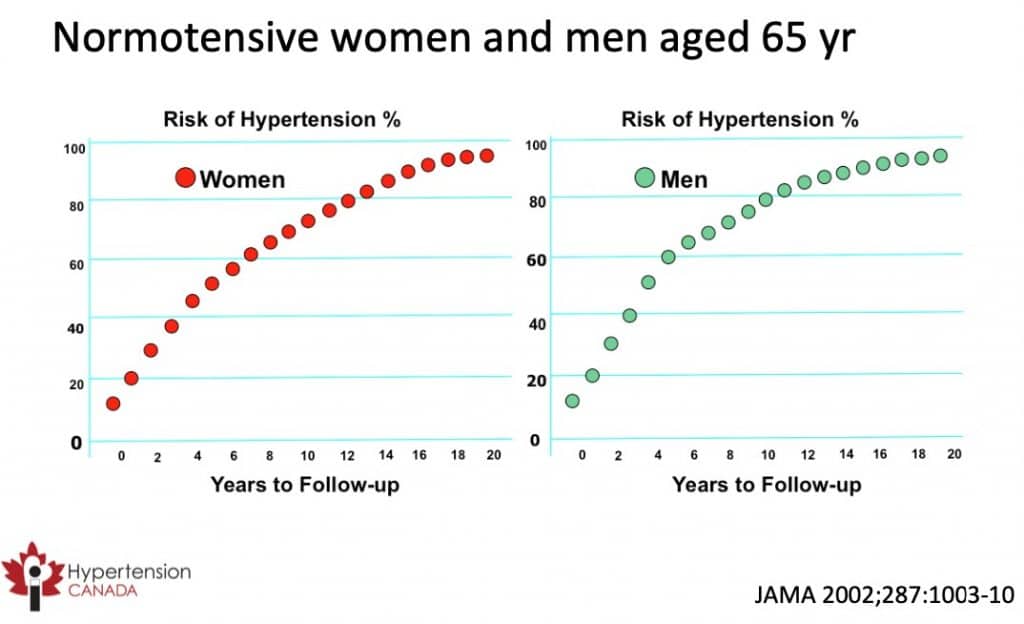
When evaluating any patient for hypertension, it is important to keep in mind risk factors that put certain patients at risk for hypertension. It is crucial to keep these risk factors in mind because even if the patient is not currently hypertensive, these risk factors can predispose the patient for hypertension later on in life. While some of these risk factors are non-modifiable, other risk factors are modifiable and can be changed in order to prevent a future diagnosis of hypertension. Some of these risk factors for hypertension include age, obesity, poor dietary habits, high sodium intake, sedentary lifestyle and high alcohol consumption.
The graphs below provide a visual depiction of the lifetime risk of hypertension in normotensive women and men aged 65 years. These visuals clearly demonstrate that hypertension risk increases significantly with age.
SECONDARY CAUSES OF HYPERTENSION
In addition to the aforementioned primary risk factors for hypertension, there are also many secondary causes of hypertension as well. These secondary causes are often underlying medical conditions or drugs/substances which can be responsible for elevating the blood pressure in certain individuals. Examples of secondary causes of hypertension include endocrine disorders (e.g. pheochromocytoma, Cushing’s syndrome, hyperthyroidism), primary hyperaldosteronism, chronic kidney disease, renovascular disease, obstructive sleep apnea, and drugs.
The table below outlines in detail some of the prescription drugs and substances which can be leading secondary causes of hypertension.
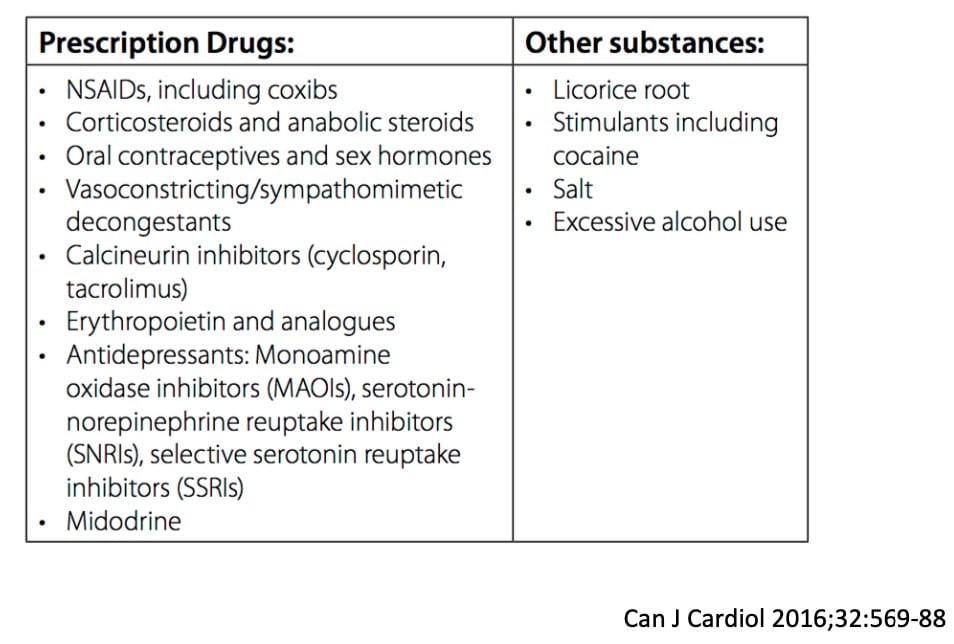
NOTE: NSAIDS include Advil, Aleve, Naproxen / CORTICOSTEROIDS include Prednisone / ORAL CONTRACEPTIVES are birth control and include Alesse, Alysena, Yasmin, Yaz / ANTIDEPRESSANTS include Fluoxetine, Sertraline, Paroxetine, Cipralex.
HYPERTENSION GUIDELINES AND WHO TO SCREEN
The latest guidelines informing pharmacotherapy decisions in the treatment of hypertension come from the Canadian Journal of Cardiology.
In terms of who to screen for hypertension, it should be noted that as per the Canadian Journal of Cardiology, “health care professionals who have been specifically trained to measure BP accurately should assess BP in all adult patients at all appropriate visits to determine CV risk and monitor antihypertensive treatment.” In addition, all patients with hypertension should undergo a cardiovascular risk assessment regardless of their age.
BLOOD PRESSURE MEASUREMENT
In terms of measuring blood pressure, it is important to use standardized techniques and validated equipment. There are Four approaches to measuring blood pressure in patients, these include office (or clinic) non-automated (auscultatory), office (or clinic) automated (oscillometric), ambulatory and home. It should also be noted that electronic (oscillometric) upper arm devices are preferred over auscultation.
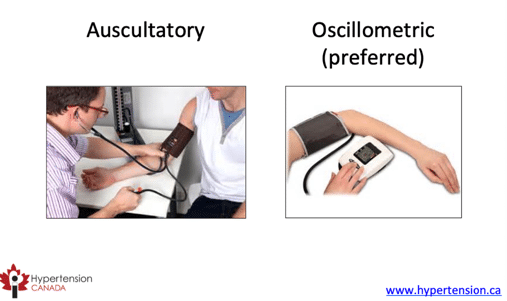
It should also be noted that auscultatory blood pressure is often inaccurate, and too rapid deflation of the cuff, digit preference (i.e. rounding to 0 or 5) or uncalibrated aneroid devices, can all lead to inaccurate measurements. Routine auscualtory blood pressure is 9/6 mmHg higher than standardized research blood pressure.
When measuring blood pressure, it is important to use a standardized technique. Seat the patient in a quiet room, set the device to take measurements at 2-minute intervals, take an initial measurement to verify that the device is registering a measurement, and leave the patient alone after the first measurement and let the device automatically takes subsequent readings. This prevents any risk of white coat hypertension.
Ambulatory blood pressure is useful for diagnosing hypertension in patients with office blood pressures above target, a fluctuating office blood pressure or suspected hypertension. In addition, home blood pressure measurement is useful in those patients with suspected non-adherence, suspected white coat hypertension or suspected masked hypertension.
Below are some resources for where to locate appropriate devices and adequate training for measuring blood pressure:
Appropriate device – List available on www.hypertension.ca
Adequate training – Video available on www.hypertension.ca
HYPERTENSION DIAGNOSIS
In beginning the diagnosis for hypertension in patients, it should be noted that all patients with new hypertension should undergo an urinalysis, serum sodium, potassium and creatinine lab work, a fasting blood glucose or hemoglobin A1C, a lipid panel and a standard 12-lead ECG.
The different target blood pressure indicative for a diagnosis of hypertension are listed blow in table format:
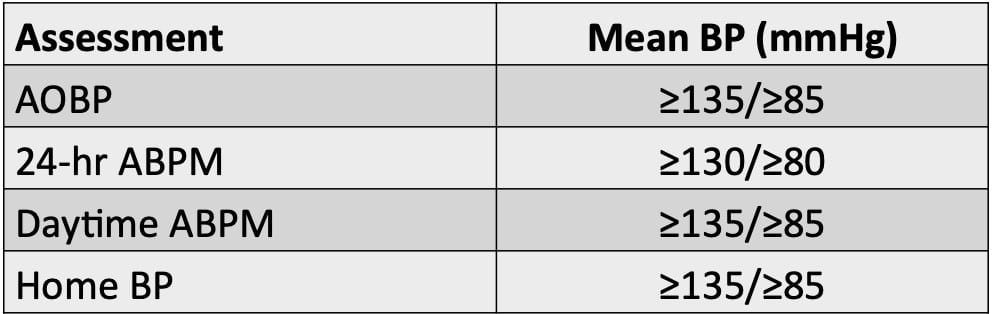
Note: AOBP is automated office blood pressure which is measured at the doctor’s office. 24hr ABPM is 24 hr ambulatory blood pressure measurement which is the average blood pressure in a 24 hour period. Daytime ABPM is average ambulatory blood pressure in the daytime. Home BP is home blood pressure.
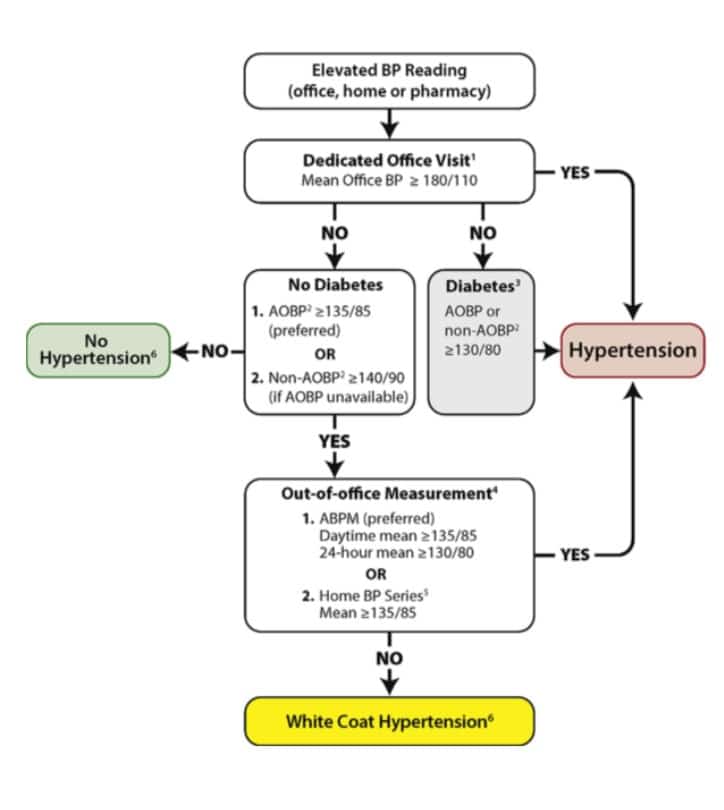
In addition, based on the Canadian Journal of Cardiology’s 2020 hypertension guidelines, the flow chart below indicated the thought process/systematic review which must be done when categorizing and diagnosing patients with hypertension.
When measuring blood pressure, it is common for there to be signs of both white coat hypertension or masked hypertension. It is important to remember that signs of white coat hypertension include women/pregnancy, older adults, recently diagnosed with hypertension with a limited number of routine office blood pressure measurements, non-smokers, mild hypertension, or no evidence of end-organ damage. Risk factors for masked hypertension include high-normal clinic blood pressure, older adults, males, higher BMI, smokers, excess alcohol consumption, diabetes mellitus, peripheral artery disease, orthostatic hypotension and left ventricular hypertrophy.
TREATMENT OF HYPERTENSION
When treating hypertension, it is important to first keep in mind patient values and preferences and then realize that the optimal approach to hypertension control will be a combination of health behaviour measures and pharmacotherapy. Ultimately, the goals of therapy are to prevent mortality and prevent morbidity. The table below outlines how a reduction in systolic blood pressure can lead to a corresponding reduction in mortality in different conditions.
HEALTH BEHAVIOUR INTERVENTIONS
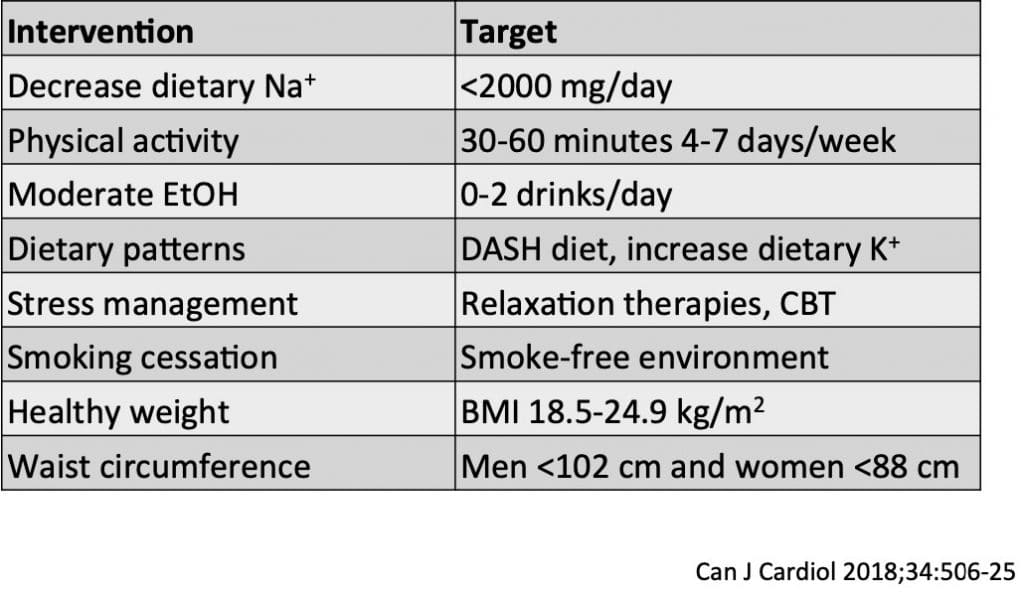
HYPERTENSION PHARMACOTHERAPY
There are many different agents which can be used to manage and control hypertension. A list of these agents is provided below:
- Angiotensin-converting enzyme inhibitors (ACEIs)
- Angiotensin receptor blockers (ARBs)
- β-blockers
- Calcium channel blockers (CCBs)
- Diuretics
- Mineralocorticoid receptor antagonists (MRAs)
- Vasodilators
- α1-blockers
- Centrally-acting agents (α2-agonists)
- Direct renin inhibitors
ANGIOTENSIN-CONVERTING ENZYME INHIBITORS (ACEIs) AND ANGIOTENSIN RECEPTOR BLOCKERS (ARBs)
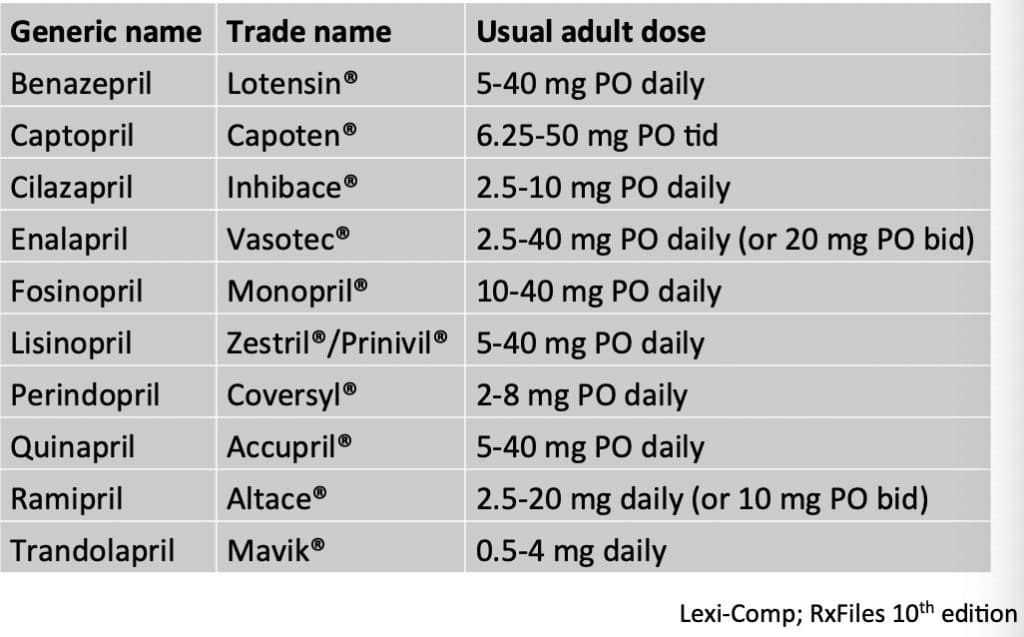
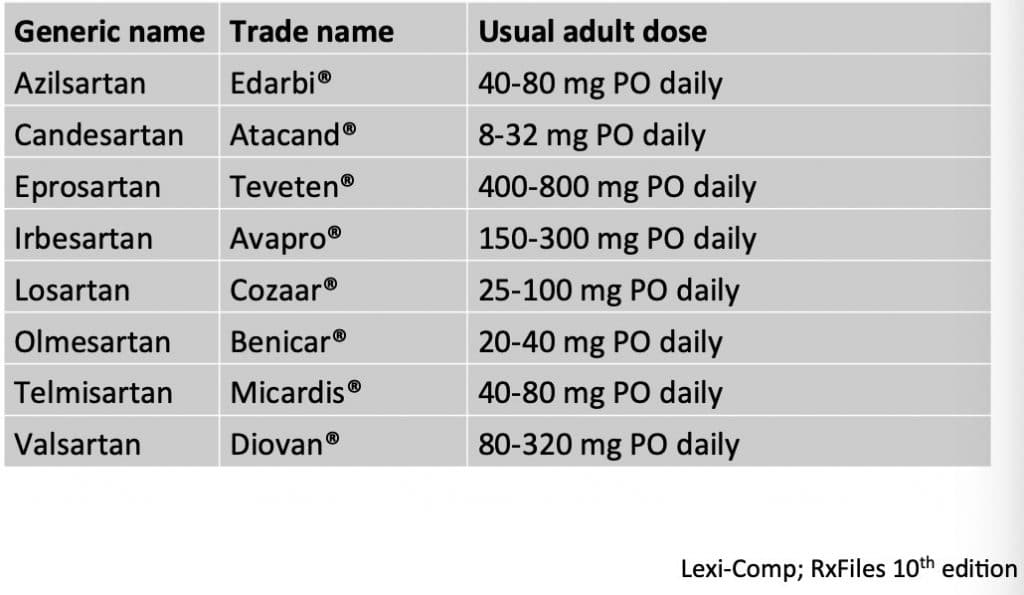
Contraindications to ACEI/ARBs:
- Bilateral renal artery stenosis
- Hypersensitivity
- Pregnancy
- History of angioedema
Side Effects:
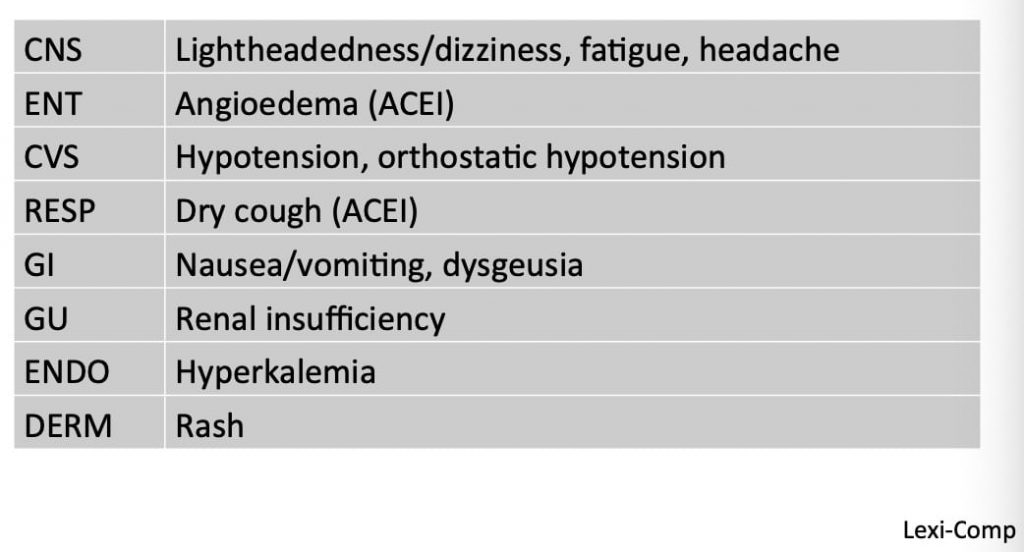
Note: angioedema is tongue swelling, hypotension is low blood pressure, orthostatic hypotension is low blood pressure upon standing, dysgeusia is change in taste, renal insufficiency is decreased kidney function and hyperkalemia is higher potassium
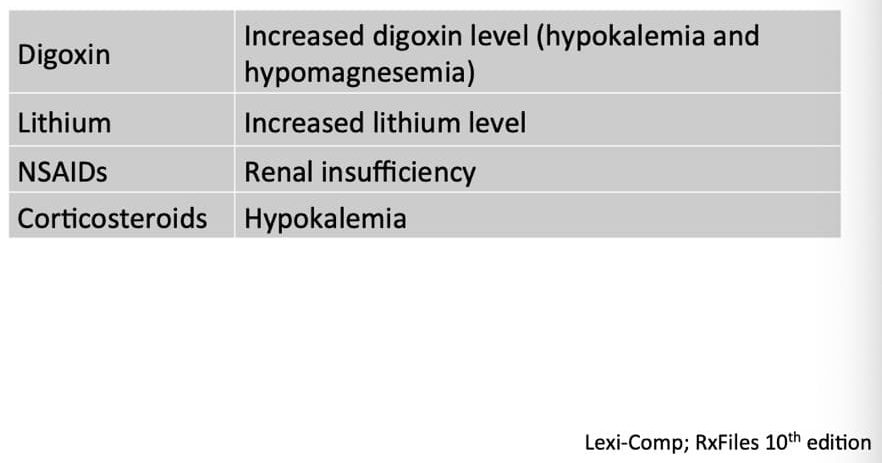
Drug Interactions:
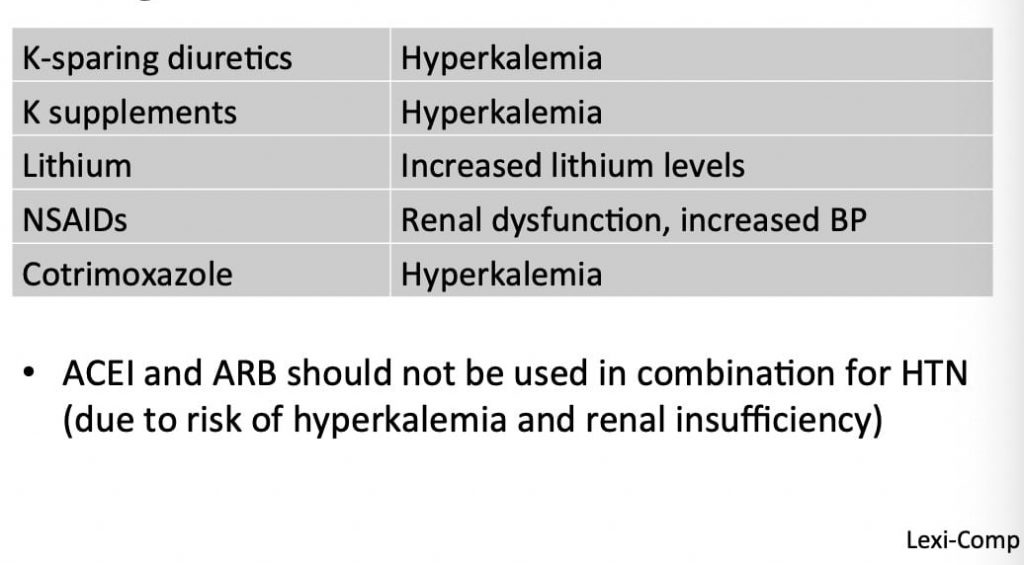
Note: Hyperkalemia is higher potassium and NSAIDs include Advil, Aleve, Naproxen etc.
BETA-BLOCKERS
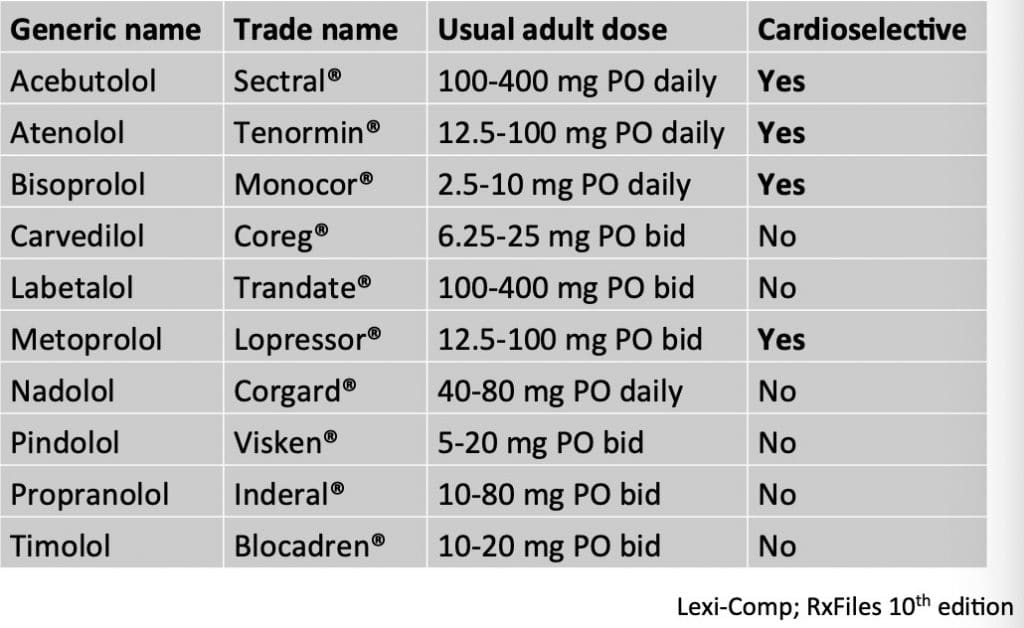
Contraindications to beta-blockers:
- Severe asthma (cardioselective beta-blockers may be safe in mild to moderate asthma)
- Secondary or tertiary heart block
- Decompensated heart failure
- Severe peripheral artery disease
- Pheochromocytoma (without alpha1 blocker)
- Hypersensitivity
Side Effects:
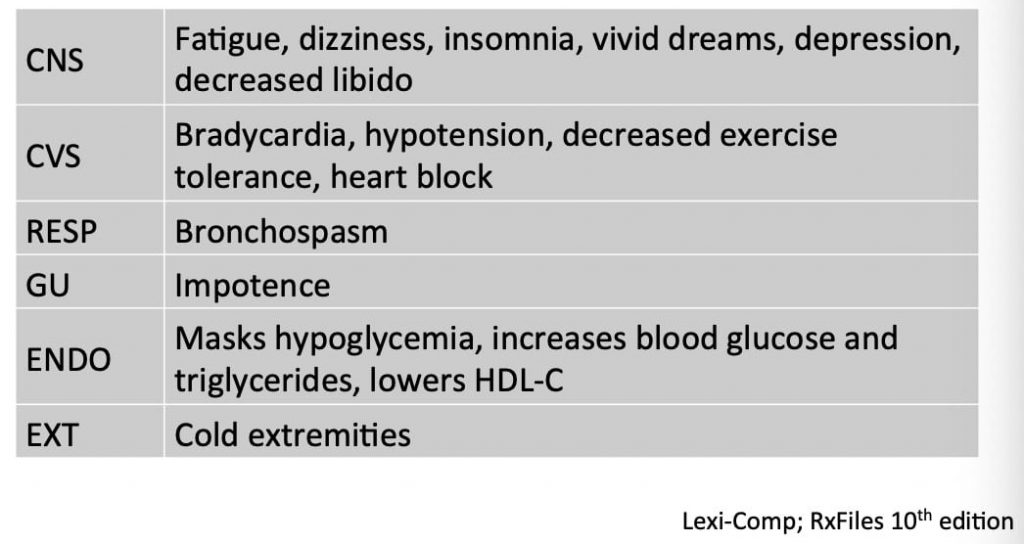
Note: bradycardia is low heart rate (less than 60 beats per minute), hypotension is low blood pressure, bronchospasm is difficulty breathing, impotence is decreased sexual function, hypoglycemia is low blood sugar
Drug Interactions:
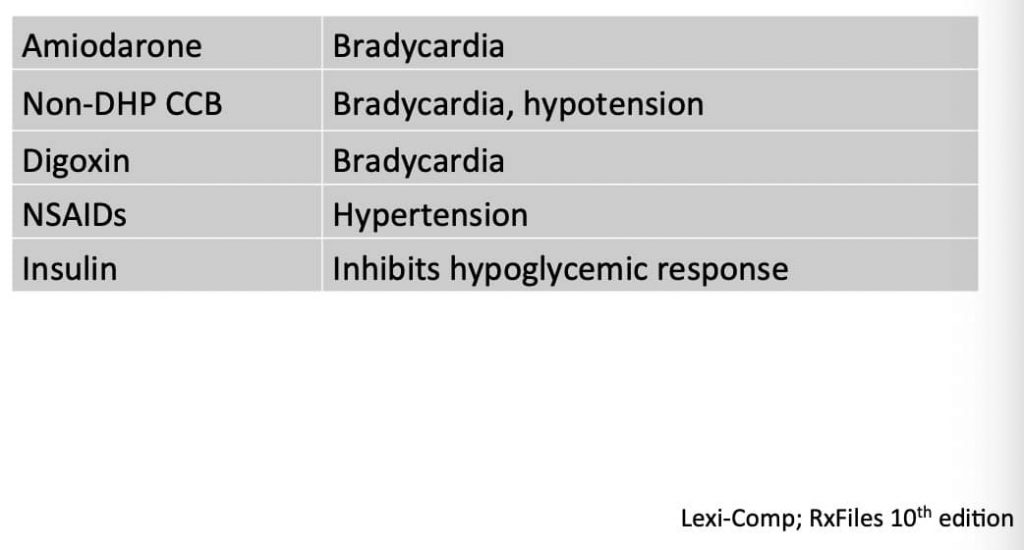
Note: bradycardia is low heart rate (less than 60 beats per minute), hypotension is low blood pressure
CALCIUM CHANNEL BLOCKERS
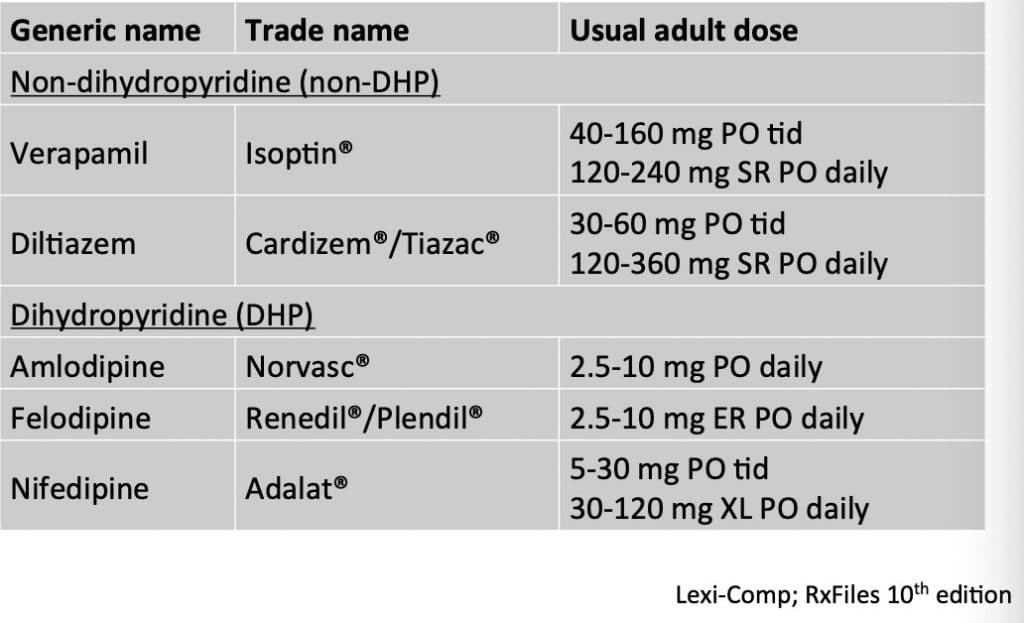
Contraindications to calcium channel blockers:
- Severe hypotension (Systolic blood pressure less than 90mmHg)
- Recent MI with pulmonary edema
- Heart failure with reduced ejection fraction (exception: amlodipine)
- Secondary or tertiary heart block or sick sinus syndrome
- Hypersensitivity
Side Effects:
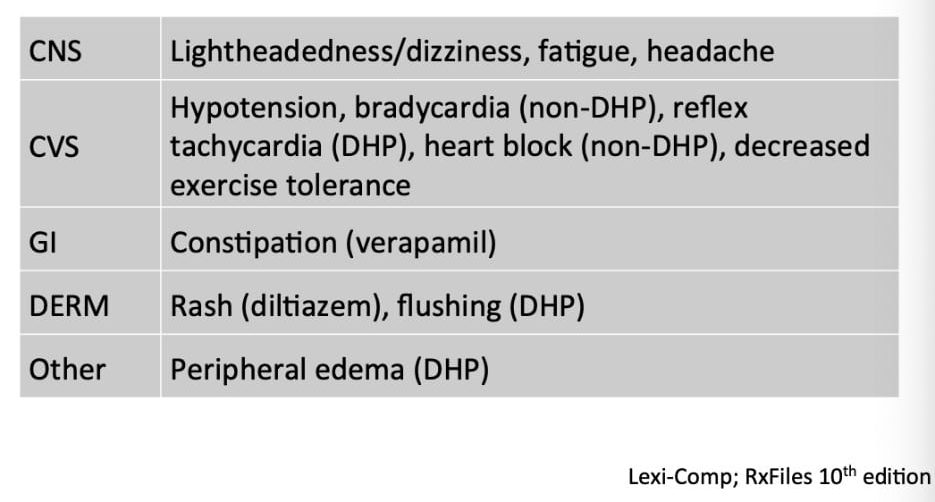
Note: hypotension is low blood pressure, bradycardia is low heart rate (less than 60 beats per minute), peripheral edema is swelling
Drug Interactions:
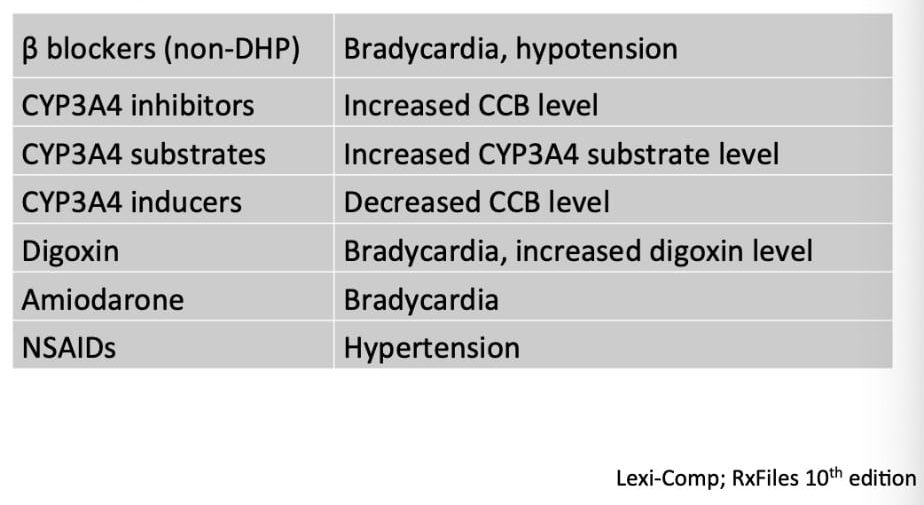
Note: bradycardia is low heart rate (less than 60 beats per minute), hypotension is low blood pressure, NSAIDs include Advil, Aleve, and Naproxen
DIURETICS
Contraindications to diuretics:
- Anuria
- Gout
- Hyponatremia
- Severe sulfa allergy
- Hypersensitivity
- Breastfeeding
Side Effects:
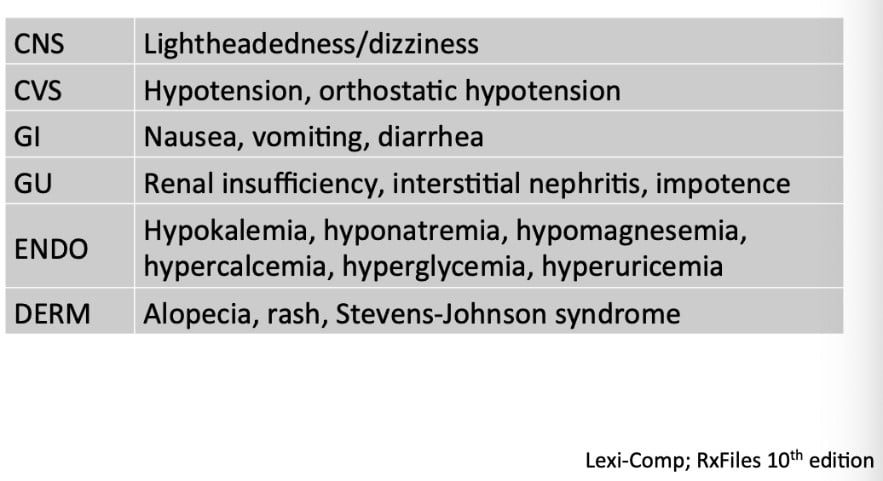
Note: hypotension is low blood pressure, orthostatic hypotension is low blood pressure upon standing, renal insufficiency is decreased kidney function, interstitial nephritis is decreased kidney function, impotence is decreased sexual function, hypokalemia is low potassium, hyponatremia is low sodium, hypomagnesemia is low magnesium, hypercalcemia is high calcium, hyperglycemia is high blood sugar, hyperuricemia is high uric acid, alopecia is hair loss and Stevens-Johnson syndrome is a skin rash.
Drug Interactions:
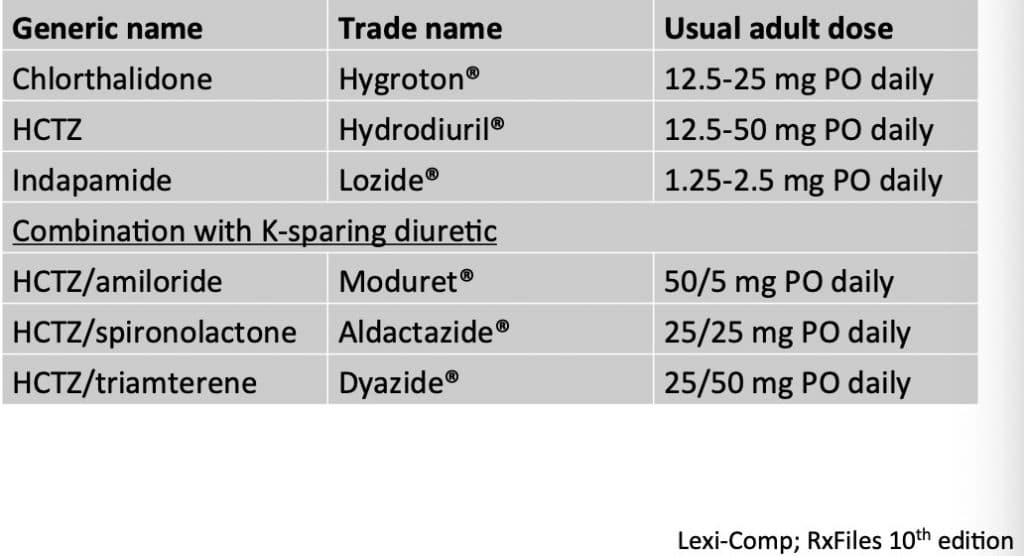
MISCELLANEOUS ANTIHYPERTENSIVE AGENTS AND USUAL ADULT DOSES
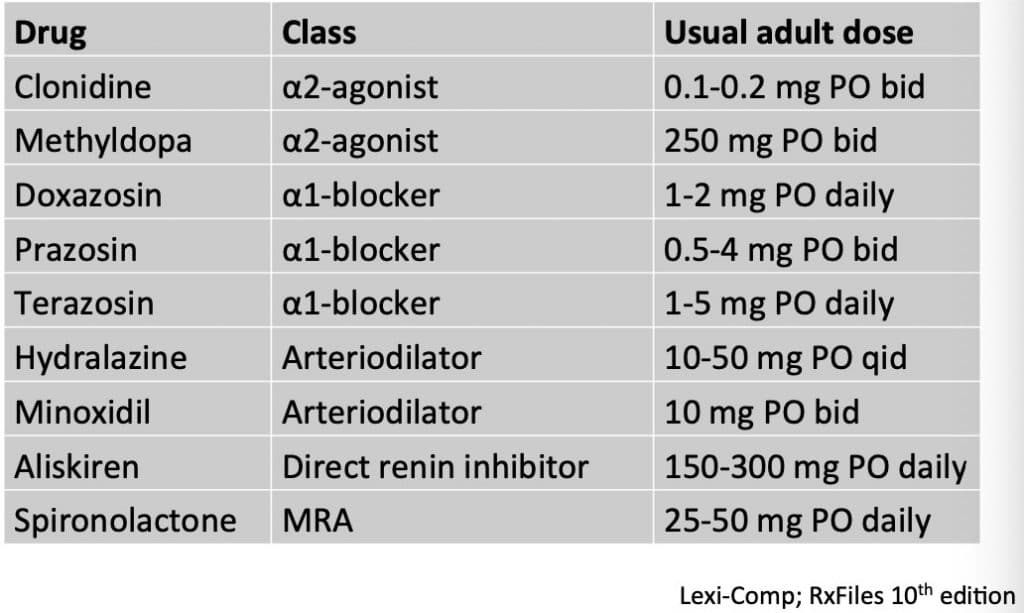
It should be noted that arteriodilators such as hydralazine and spironolactone are used in the treatment of resistant hypertension when first line agents have failed. Ateriodilators are preferred over spironolactone in cases where electrolyte balance of potassium is a concern. Alpha agonists and blockers are used in combination with agents such as diuretics to control hypertension, and alpha agonists are preferred in instances where orthostatic hypotension is a concern for patients. Aliskiren is no longer used anymore.
BLOOD PRESSURE TARGETS
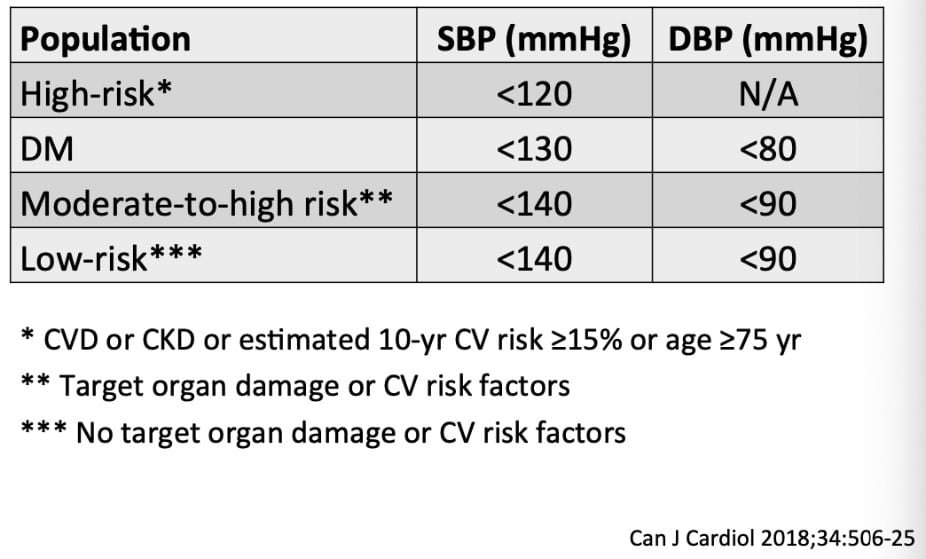
It should be noted that blood pressure targets vary depending on both the age of the patient and any other underlying health conditions. It should also be taken into consideration that in certain elderly population (age 70 years and older) or those patients on palliative care, that the blood pressure is often let to run higher than the usual target since the holistic goals of therapy for that respective patient want to be taken into consideration.
ALGORTHM FOR CHOOSING WHICH HYPERTENSIVE AGENT TO START
When choosing which antihypertensive agents to choose, a simple algorithm can be followed in order to ensure that the chosen pharmacotherapy is both effective and safe for the patient.
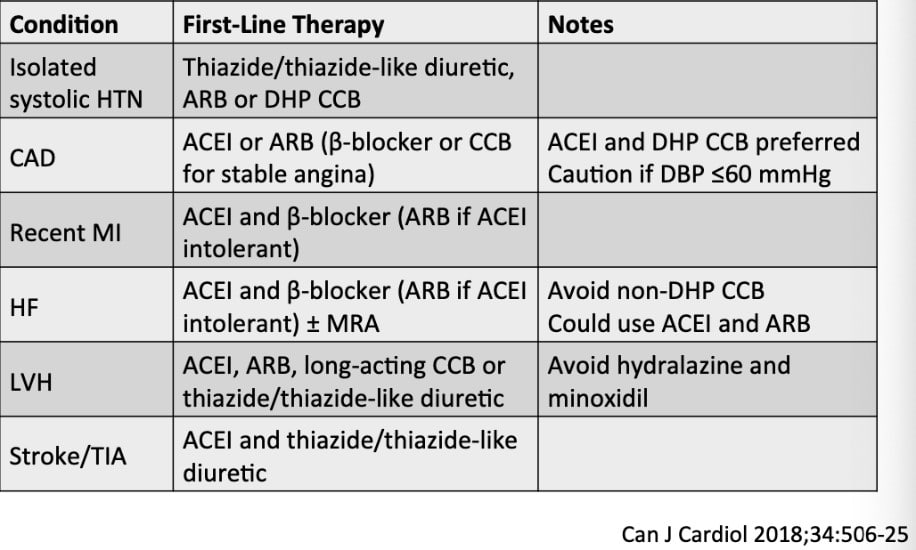
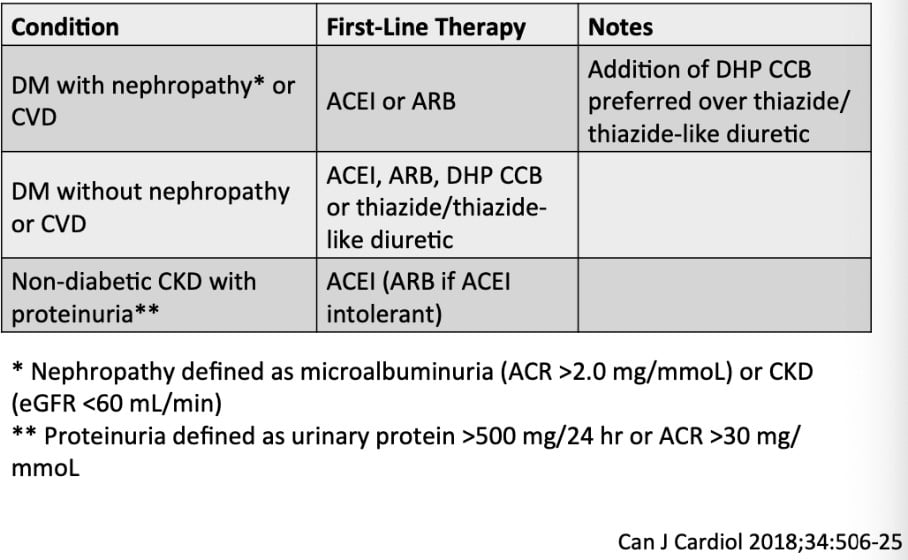
STEP 1: When choosing an antihypertensive agent, first consult the below table to choose an antihypertensive agent which is INDICATED and EFFECTIVE given the patient’s underlying medical conditions.
STEP 2: Once an agent has been chosen, consult the aforementioned list of contraindications, side effects and drug interactions for that agent in order to ensure that the chosen agent is SAFE for the patient. (these are listed previously in this blog post)
STEP 3: Take into consideration miscellaneous “therapeutic pearls” when finalizing your decision as listed below:
- Long acting diuretics like indapamide and chlorthalidone are preferred over shorter acting diuretics like hydrochlorothiazide
- Beta-blockers are not indicated as first line therapy for age 60 and above
- Recommended single pill combinations are those with an ACEI and a CCB, or ARB and a CCB or ACEI/ARB and a diuretic
- Multiple drugs are often required to reach target levels especially in patients with type 2 diabetes
- Reassess patients with uncontrolled blood pressure at least every 2 months
DRUG-INDUCED NUTRIENT DEPLETION (SPECIFIC TO ANTIHYPERTENSIVES)
|
Antihypertensive Agent |
Nutrient |
|
Acebutolol |
CoQ10 |
|
Amiloride |
Folic Acid, Calcium |
|
Amiloride and HCTZ |
Magnesium, Phosphorus, CoQ10, Potassium, Sodium, Zinc |
|
Atenolol and Chlorthalidone |
Magnesium, Phosphorus, CoQ10, Potassium, Sodium, Zinc |
|
Benazepril |
Zinc |
|
Bisoprolol |
CoQ10 |
|
Candesartan and HCTZ |
CoQ10, Zinc, Potassium, Sodium, Phosphorus, Magnesium |
|
Captopril |
Zinc |
|
Carvedilol |
CoQ10 |
|
Thiazide Diuretics |
Sodium, CoQ10, Zinc, Potassium, Phosphorus, Magnesium |
|
Enalapril |
Zinc, B Complex Vitamins, Sodium, Potassium, Phosphorus, Magnesium, CoQ10 |
|
Furosemide |
Calcium, Magnesium, Potassium, Sodium, B Complex Vitamins, Vitamin C, Zinc |
|
Hydrochlorothiazide |
Sodium, Potassium, Zinc, Magnesium, Phosphorus, CoQ10, Calcium, Folic Acid |
|
Indapamide |
CoQ10, Magnesium, Zinc, Sodium, Potassium, Phosphorus |
|
Irbesartan and HCTZ |
Sodium, Zinc, Magnesium, Phosphorus, Calcium, Potassium, CoQ10 |
|
Lisinopril |
Zinc |
|
Metolazone |
Sodium, CoQ10, Magnesium, Phosphorus, Potassium, Zinc |
|
Metoprolol |
CoQ10 |
|
Prazosin and Polythiazide |
Potassium, Phosphorus, Magnesium, CoQ10, Sodium, Zinc |
|
Propranolol |
CoQ10, Magnesium, Phosphorus, Potassium, Sodium, Zinc |
|
Quinapril |
Zinc |
|
Ramipril |
Zinc |
|
Sotalol |
CoQ10 |
|
Telmisartan and HCTZ |
Sodium, Zinc, Potassium, Phosphorus, Magnesium, CoQ10 |
|
Timolol |
CoQ10 |
|
Trandolapril and Verapamil |
Zinc |
|
Valsartan and HCTZ |
Sodium, Zinc, Potassium, Phosphorus, Magnesium, CoQ10 |
Note: For every drug that depletes CoQ10, there needs to be an added 100mg of supplemental CoQ10 added.
ADDENDUM: EXPLANATION OF ALPHA AND BETA RECEPTORS
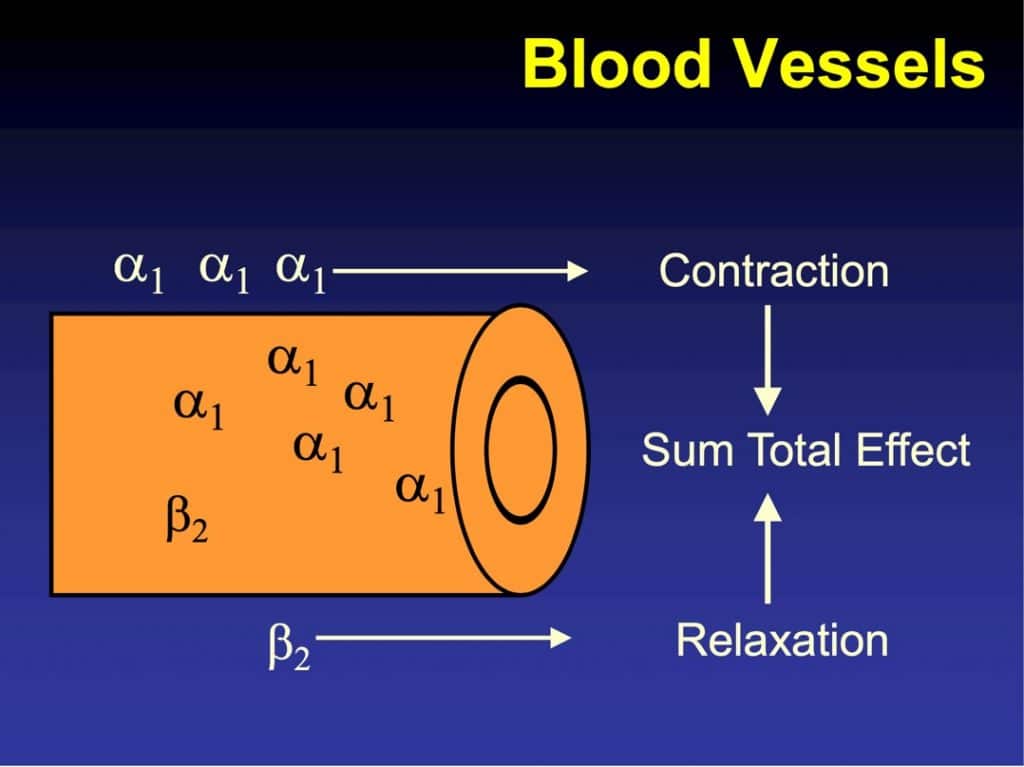
- ALPHA 1 receptor: norepinephrine binds alpha 1 receptors to cause blood vessel contraction and increased blood pressure; alpha 1 blockers thus block the norepinephrine binding and dilate blood vessels
- ALPHA 2 receptor: mainly found in the brain stem and alpha 2 agonists cause a reduction of sympathetic outflow and thus reduced blood pressure
- BETA 1 receptor: mainly found on the heart and beta blockers slow heart rate and decrease blood pressure
- BETA 2 receptor: mainly found on bronchioles and have minimal effect on lowering heart rate/blood pressure as with the beta 1 selective blockers
REFERENCES:
- Rabi DM, McBrien KA, Sapir-Pichhadze R et al. Hypertension Canada’s 2020 comprehensive guidelines for the prevention, diagnosis, risk assessment, and treatment of hypertension in adults and children. Can J Cardiol2020;36(5):596-624.
- CPS [Internet]. Ottawa, ON: Canadian Pharmacists Association; 2019 [cited 2021 Jan 17]. Hypertension. Available from: http://www.e-therapeutics.ca. Also available in paper copy from the publisher.
- CPS [Internet]. Ottawa, ON: Canadian Pharmacists Association; 2019 [cited 2021 Jan 17]. Angiotensin Converting Enzyme Inhibitors. Available from: http://www.e-therapeutics.ca. Also available in paper copy from the publisher.
- CPS [Internet]. Ottawa, ON: Canadian Pharmacists Association; 2019 [cited 2021 Jan 17]. Angiotensin Receptor Blockers. Available from: http://www.e-therapeutics.ca. Also available in paper copy from the publisher.
- CPS [Internet]. Ottawa, ON: Canadian Pharmacists Association; 2019 [cited 2021 Jan 17]. Beta Blockers. Available from: http://www.e-therapeutics.ca. Also available in paper copy from the publisher.
- CPS [Internet]. Ottawa, ON: Canadian Pharmacists Association; 2019 [cited 2021 Jan 17]. Calcium Channel Blockers. Available from: http://www.e-therapeutics.ca. Also available in paper copy from the publisher.
- CPS [Internet]. Ottawa, ON: Canadian Pharmacists Association; 2019 [cited 2021 Jan 17]. Diuretics. Available from: http://www.e-therapeutics.ca. Also available in paper copy from the publisher.
- CPS [Internet]. Ottawa, ON: Canadian Pharmacists Association; 2019 [cited 2021 Jan 17].Clonidine. Available from: http://www.e-therapeutics.ca. Also available in paper copy from the publisher.
- CPS [Internet]. Ottawa, ON: Canadian Pharmacists Association; 2019 [cited 2021 Jan 17].Methyldopa. Available from: http://www.e-therapeutics.ca. Also available in paper copy from the publisher.
- CPS [Internet]. Ottawa, ON: Canadian Pharmacists Association; 2019 [cited 2021 Jan 17]. Doxazosin. Available from: http://www.e-therapeutics.ca. Also available in paper copy from the publisher.
- CPS [Internet]. Ottawa, ON: Canadian Pharmacists Association; 2019 [cited 2021 Jan 17]. Prazosin. Available from: http://www.e-therapeutics.ca. Also available in paper copy from the publisher.
- CPS [Internet]. Ottawa, ON: Canadian Pharmacists Association; 2019 [cited 2021 Jan 17].Terazosin. Available from: http://www.e-therapeutics.ca. Also available in paper copy from the publisher.
- CPS [Internet]. Ottawa, ON: Canadian Pharmacists Association; 2019 [cited 2021 Jan 17]. Hydralazine. Available from: http://www.e-therapeutics.ca. Also available in paper copy from the publisher.
- CPS [Internet]. Ottawa, ON: Canadian Pharmacists Association; 2019 [cited 2021 Jan 17].Minoxidil. Available from: http://www.e-therapeutics.ca. Also available in paper copy from the publisher.
- CPS [Internet]. Ottawa, ON: Canadian Pharmacists Association; 2019 [cited 2021 Jan 17].Aliskiren. Available from: http://www.e-therapeutics.ca. Also available in paper copy from the publisher.
- CPS [Internet]. Ottawa, ON: Canadian Pharmacists Association; 2019 [cited 2021 Jan 17]. Spironolactone. Available from: http://www.e-therapeutics.ca. Also available in paper copy from the publisher.
- National Vitamin Company. Drug-Induced Nutrient Depletion Guide [pamphlet]. Arizona.